www.buildingsandcities.org/insights/commentaries/from-sars-to-covid-19-and-beyond.html
From SARS to COVID-19 and Beyond: Public Health Lessons for Buildings
The built environment has a fundamental role in maintaining public health. What lessons has Hong Kong applied to reduce the spread of contagion?
An important function of the built environment
is providing a safe place for its inhabitants.
Edward Ng (Chinese University of Hong Kong) recalls the spread of SARS in Hong Kong and reflects on the public health lessons for the built environment. A process of preparation and management is vital for
reducing present and future health risks. This is becoming evident in Hong Kong's
recent codes and regulations for urban design and buildings . Other cities can learn from this process.
Background
Dr Liu (patient zero) arrived in Hong Kong from Guangdong in February 2003. He stayed in a hotel downtown. It was a small and busy hotel. Dr Liu was not well and was coughing. Little did he realize that he infected 9 others in the confined spaces of the hotel -- lobby, lifts and corridors. Dr Liu died on 4 March 2003. The 9 individuals he infected, mostly tourists, later left Hong Kong and subsequently caused the worldwide outbreak of SARS where more than 2300 people in 17 countries were infected eventually. 80 lives were lost. (HKSARG, 2003)
Within a month, SARS rapidly spread to Hong Kong population (Lee, 2003). Amoy Gardens is a typical housing estate the metro area in Hong Kong. Soon after the first case was reported on 14 March, more than 300 cases were recorded by early April; they were mostly concentrated in 3 building blocks closely located to each other.
Subsequent studies reveal that the diseases spread from the toilet of an inhabitant on the 16th floor in Block E into the re-entrant space, and travelled upward to the other floors (Figure 1).
The widely reported saga was the most important wakeup call for policy makers, regulators, stakeholders, developers, planners and architects in Hong Kong. The media message to the general public was clear: the planning and design of buildings is an important consideration for healthy living.
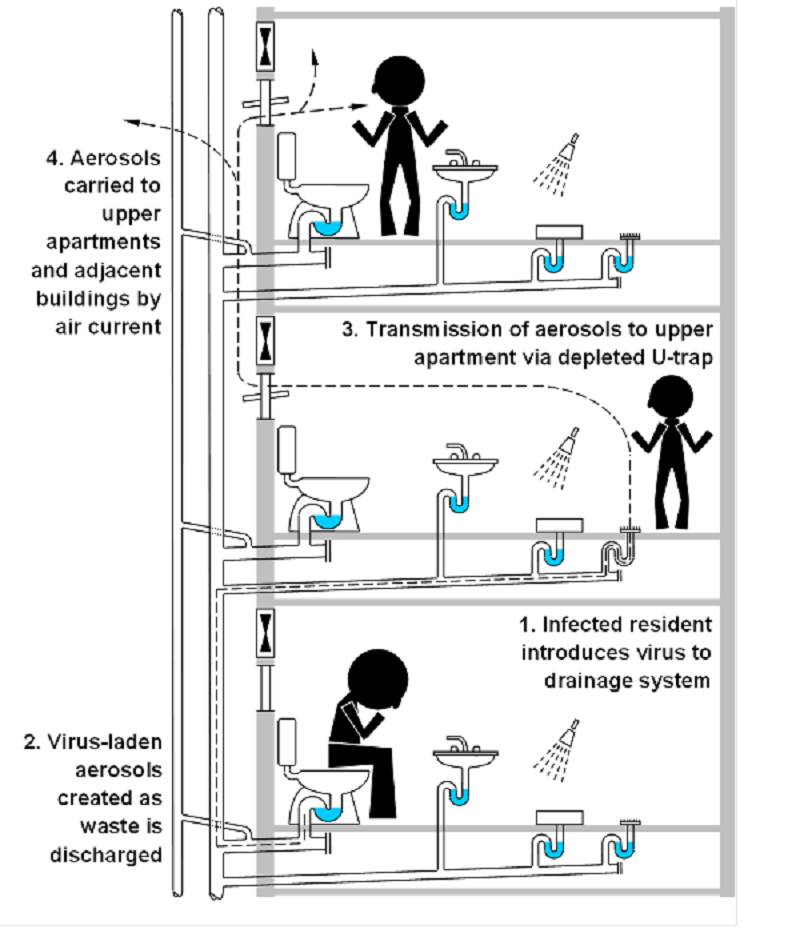
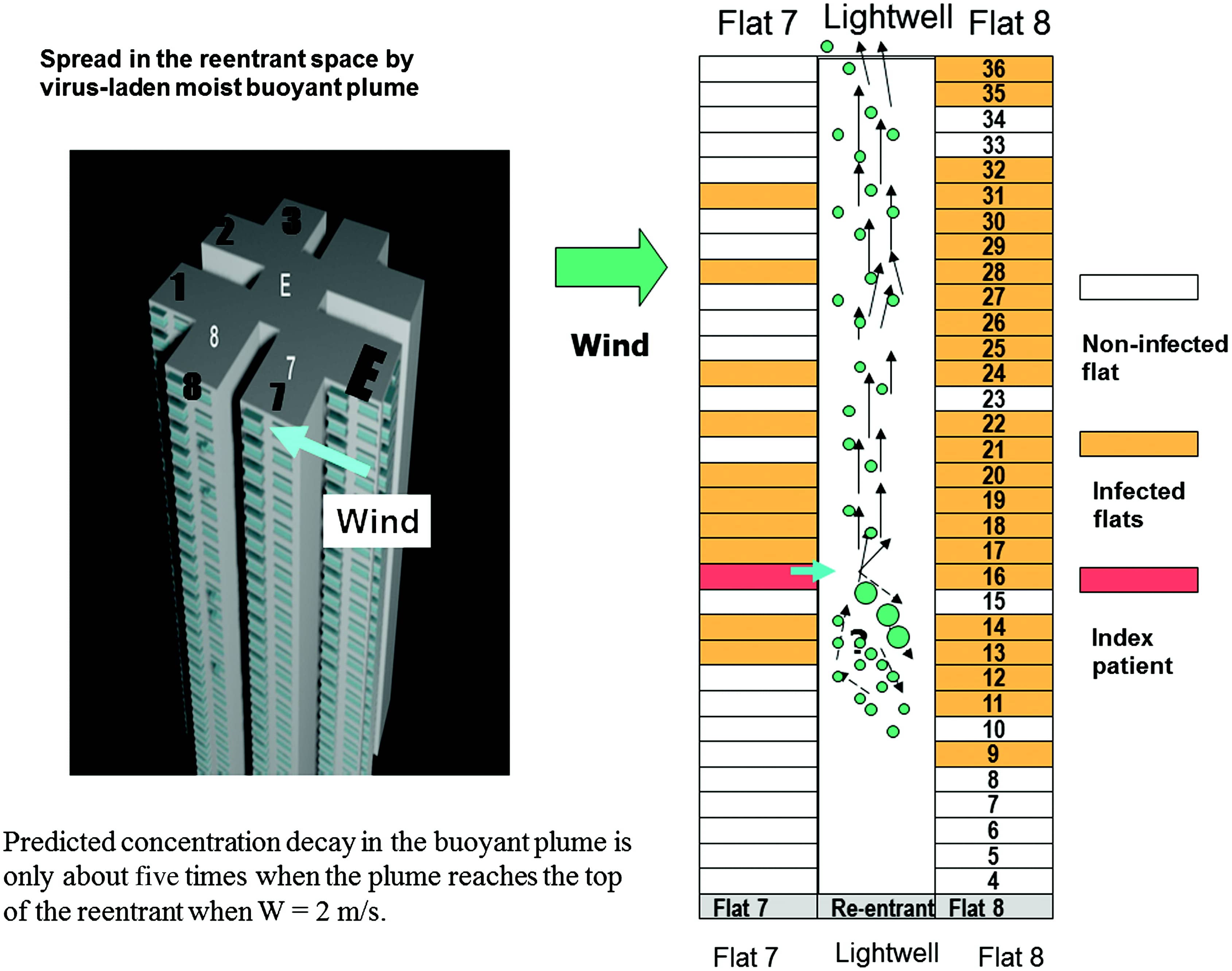
FIGURE 1. LEFT: The spread of the SARS contagion through buildings was only revealed by research after the epidemic subsided. The infection spread to the occupants via the vertical drainage pipe. This then spread to the occupants on the floors above via windows. (Gormley et al., 2017) CENTRE and RIGHT: Contaminated droplets from the 16th floor escaped and were carried via buoyancy effect to the other floors. (Lee, 2012)
Changes to policy after SARS
After the SARS episode subsided, the Government of Hong Kong Special Administrative Region (HKSAR) began an investigation into the spread of SARS (to learn the lessons from the Amoy Gardens) in order to reduce future risks. It established a Team Clean Commission to coordinate the efforts (Team Clean, 2003). One of the Commission's recommendations was that outdoor air circulation should be factored into future planning and design practices. The other recommendation was that planners should evaluate and establish the city's air circulation capacity and its relationship with the city's development densities and building layouts. The public health basis for the recommendations was to improve ventilation of indoor and outdoor spaces so as to quickly mix the contaminated air and dilute its germ concentration, and thereby prevent spread of disease due to cross contamination in confined spaces (Nielsen, 2009; McKinney et al., 2006).
To address the faulty drainage design, the Buildings Department of the HKSAR Government issued new Practice Notes for Authorised Persons (PNAP=App93). The new W-trap design would prevent the drying of the water seal in the floor U trap (BD, 2014). In addition, two important building and urban design guidelines were promulgated. The first was the Air Ventilation Assessment (AVA) Technical Circular (DevB, 2006); the other was a new chapter on city-building ventilation principles in the Hong Kong Planning Standard and Guidelines (HKPSG). These two documents have since guided the construction industry in Hong Kong towards planning and designing a healthier city for high density living.
The first building project that made reference to the Technical Circular and the new chapter on city-building ventilation in the HKPSG was the Hong Kong Government Headquarters building in Tamar. The large opening responded to the computational fluid dynamics (CFD) and wind tunnel test results to improve microclimatic conditions.

FIGURE 2. The Tamar Hong Kong SAR Government Headquarters designed to Air Ventilation Assessment Technical Circular and HK Planning Standards and Guidelines for better urban ventilation (ArchDS, 2013).
SARS was not the only alarm to the construction industry stakeholders and policy makers in the history of Hong Kong. In 1894, Hong Kong suffered the deadlier Bubonic Plague that eventually killed more than 20,000 people. British sanitary engineer Osbert Chadwick evaluated the situation and recommended that the poor sanitary standard and the overcrowded living environment were the key concerns. In particular, he pointed to the lack of fresh air and sunlight in narrow streets and poorly designed back-to-back houses. In 1903, the Hong Kong Government enacted the Public Health and Building Ordinance to regulate the city. Some metro areas of the city were re-built according to the new regulations. In hindsight, the urban structure of metro Hong Kong has become what it is today mainly because of this 1903 Public Health and Building Ordinance, which was a response to the 1894 Bubonic Plague.
COVID-19
As this commentary is being written, COVID-19 is still with us. By April 2020, more than 2 million cases and over 120,000 deaths worldwide have been reported. The world is still fighting the pandemic. Lessons from how the HKSAR Government fought SARS are currently being applied: the borders are controlled, travel is restricted, gatherings are prohibited, stay home orders are issued, schools are closed, and people are advised to wear face masks, to wash hands more often and to keep a safe distance from each other. All the public health precautionary measures are in place.
Unlike SARS in 2003, COVID-19 lingers much longer and affects more countries in the world. As such, the above precautionary public health measures will be with us longer. Apart from the economic problems that governments around the world are now trying to solve, the construction industry stakeholders and policy makers are beginning to talk about how we can design a more "disease resilient" and healthier built environment. For researchers in the field of buildings and cities, there are scholarly implications that are worth pondering over, and the subject matter requires further research.
Towards healthy (disease resilient) buildings and cities
How can our buildings and cities be designed to provide physically healthy and "disease resilient" indoor and outdoor spaces? From the built environmental perspective, public health doctors have repeatedly reminded us these three keywords: "distance", "fresh air" and "sunlight".
How can our buildings and cities be designed to provide mentally healthy spaces to cope with future episodes? Isolation and quarantine may be necessary during a pandemic, but are unpleasant and difficult experiences. Environmental psychologists have pointed to three key built environmental provisions that are spatially related: "social interaction", "nature & openness" and "exercise".
The precise definitions and metrics of these six keywords will require further evidence. These insights will provide additional meanings and precautions when designing our buildings and cities for health and wellness, green, sustainable, low carbon, resilient, regenerative criteria.
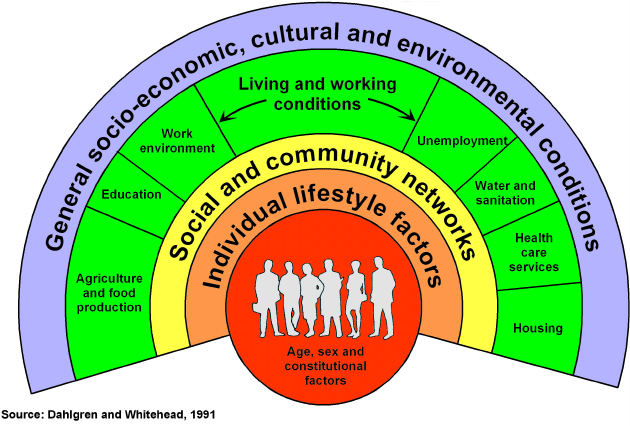
The World Health Organisation's definition of a healthy city is a useful starting point:
"one that is continually creating and improving those physical and social environments and expanding those community resources which enable people to mutually support each other in performing all the functions of life and in developing to their maximum potential." (WHO, 1998)
The definition is broad and it is often graphically represented as The Rainbow Model. There are many issues that are related to buildings and cities. WHO's holistic model would allow every city to develop its own priorities and balance its focuses.
Based on this model, this understanding can be contextualised for policy makers in Hong Kong:
- Land use: Hong Kong's rapid urbanisation has challenged policy makers to seek a balance between the urban, suburban and periurban relationship in terms of land use and land utilization. For example, the debates on whether to develop our country parks is still on-going. During SARS and COVID-19, locals take refuge in Hong Kong's country parks for fresh air and the enjoyment of nature. The health benefits of our country parks require further quantification and re-valuation.
- Density: Hong Kong is notable for its high-density urban living environment and its lack of green open spaces. Key design issues for planners, urban designers and architects are how to design our buildings for high density living whilst avoiding close social contact and/or cross contamination. In addition, how can the quality and experience of urban green open spaces be enhanced to provide relief for locals living under a quarantined condition or during extreme heat events?
- Ageing society: In 20 years a third of Hong Kong's population will be 65 and above. Our elderly population is the most vulnerable to COVID-19 and any future diseases. What can be done now in policy and practice to incorporate the lessons learned in SARS and COVID-19 to design a more "disease resilient" living environment?
- Climate Change: Epidemiologists (Patz, 2000) have already warned that new and unknown diseases will appear. For example, Dengue Fever cases in Hong Kong used to be imported from the Tropics. However, recently more local cases have been reported. WHO (2003) has already warned of an apparent increase in many infectious diseases. It is therefore likely that pandemics similar to COVID-19 will appear more often, will be more intense and will last longer.
Furthermore, beyond diseases, the hotter and more extreme environment as a result of climate change will bring further heat-stress mortality (Lee, 2011). To migrate 1 C higher urban air temperature, the ventilation flow rate needs to increase by 0.4 m/s (Höppe, 1999). Future buildings and cities need to be designed to improve microclimate and ventilation at the urban, neigbourhood and street levels.
In summary, how we design our buildings and cities to address the six keywords -- "distance", "fresh air" and "sunlight", "social interaction", "nature & openness" and "exercise" - will be topical questions for scholars.
References
ArchSD (2013). Sustainability Report. Architectural Services Department, HKSAR Government.
BD (2014). Planning and Design of Drainage Works. Practice Note for Authorized Persons, Registered Structural Engineers and Registered Geotechnical Engineers (APP-93), Buildings Department, HKSAR Government. https://www.bd.gov.hk/doc/en/resources/codes-and-references/practice-notes-and-circular-letters/pnap/APP/APP093.pdf
Dahlgren G and Whitehead M (1991). Policies and Strategies to Promote Social Equity in Health. Stockholm: Institute for the Futures Studies; 2007:14. ISSN: 1652-120X
DevB (2006). Air Ventilation Assessments Technical Circular 1/06. HKSAR Government. https://www.devb.gov.hk/filemanager/technicalcirculars/en/upload/15/1/jtc-2006-01-0-1.pdf
Gormley M, Aspray T J, Kelly D A and Rodriguez-Gil C (2017). Pathogen cross-transmission via building sanitary plumbing systems in a full scale pilot test-rig, PLoS ONE 12(2): e0171556. https://doi.org/10.1371/journal.pone.0171556
HKSARG (2003). Report on SARS in Hong Kong: from Experience to Action. SARS Expert Committee. https://www.sars-expertcom.gov.hk/english/reports/reports/reports_fullrpt.html
Höppe P (1999). The physiological equivalent temperature - a universal index for the biometeorological assessment of the thermal environment. International Journal of Biometeorology, 43: 71-75.
Lee J H W (2012). Mixing of Multiple Buoyant Jets. Journal of Hydraulic Engineering, 138:12.
Lee S H (2003). The SARS epidemic in Hong Kong: what lessons have we learned? Journal of the Royal Society of Medicine, 96(8): 374-378. doi: 10.1258/jrsm.96.8.374.
Lee T C, Chan K Y and Ginn W L (2011). Projection of extreme temperatures in Hong Kong in the 21st century. Acta Meteorologica Sinica, 25: 1-20.
Nielsen PV (2009). Control of airborne infectious diseases in ventilated spaces. Journal of the Royal Society Interface, 6(Suppl 6): S747-S755. https://doi.org/10.1098/rsif.2009.0228.focus
McKinney KR, Gong Y Y and Lewis T G (2006). Environmental transmission of SARS at Amoy Gardens. Journal of Environmental Health, 68(9):26-30.
Patz, J.A., et al. (2000). Effects of environmental change on emerging parasitic diseases. International Journal of Parasitology, 30(12-13): 1395-405.
PlanD (2015). Urban Design Guidelines, Hong Kong Planning
Standard and Guidelines. Planning Department, HKSAR Government. https://www.pland.gov.hk/pland_en/tech_doc/hkpsg/full/pdf/ch11.pdf
Team Clean (2003).
Progress of measures to improve environmental hygiene in HK. https://www.legco.gov.hk/yr03-04/chinese/hc/papers/shc0702-tcrpt-ce-scan.pdf
WHO (1998). Health Promotion Glossary. https://www.who.int/healthpromotion/healthy-cities/en/
WHO (2003). Climate change and human health - risks and responses. ISBN 9241590815.